


Why I built a website to track my own heart condition
In January 2026, I woke up at 3am with my heart doing something it had no business doing.
Not racing exactly. More like a washing machine on a spin cycle, erratic, forceful, completely out of rhythm. I lay there in the dark and thought: this again.
My first episode had been in August 2021. I’d been leaning out of a window - an awkward position that put pressure on my ribs and felt my heart flip into chaos. I was 33. My GP had never seen AFib in someone my age without an underlying cause. My cardiologist ran every test going. ECG, stress MRI, blood tests, a two-week Holter monitor. All normal. The diagnosis was paroxysmal, lone AFib, vagally mediated. Basically: your heart misfires sometimes, we don’t fully understand why, and the research on people like you is thin on the ground.
The second episode came four and a half years later, after a hot bath. Different trigger, same chaos.
When I saw my electrophysiologist, he was straightforward with me. He said I would have another episode at some point, but couldn’t tell me when. He told me I could continue to exercise. What he didn’t say, which matters and which I want to be clear about here, is that my AFib is progressive. That word gets thrown around a lot online, usually in the context of structural AFib, where it often does worsen over time. Lone AFib is a different animal. But the honest answer is that the data on long-term outcomes for young, lone AFib patients is sparse. Nobody could tell me with confidence what my condition would look like in ten years.
That’s the problem I decided to do something about.
The research gap nobody talks about
AFib affects around 1.4 million people in the UK. The vast majority are older, often with high blood pressure, heart disease, obesity, or diabetes. The clinical guidelines, the treatment protocols, the medication thresholds, all of it is built on data from that population.
Which is fine, if you’re that population.
But if you’re 37, running 40km a week, with a resting heart rate of 48 and a VO2 max of 57 (Superior category for my age and sex), the research wasn’t designed with you in mind. When I asked my cardiologist what the evidence said about training load and AFib recurrence in people like me, he paused and said there isn’t much data on that.
He’s not wrong. The data genuinely doesn’t exist.
So I built it
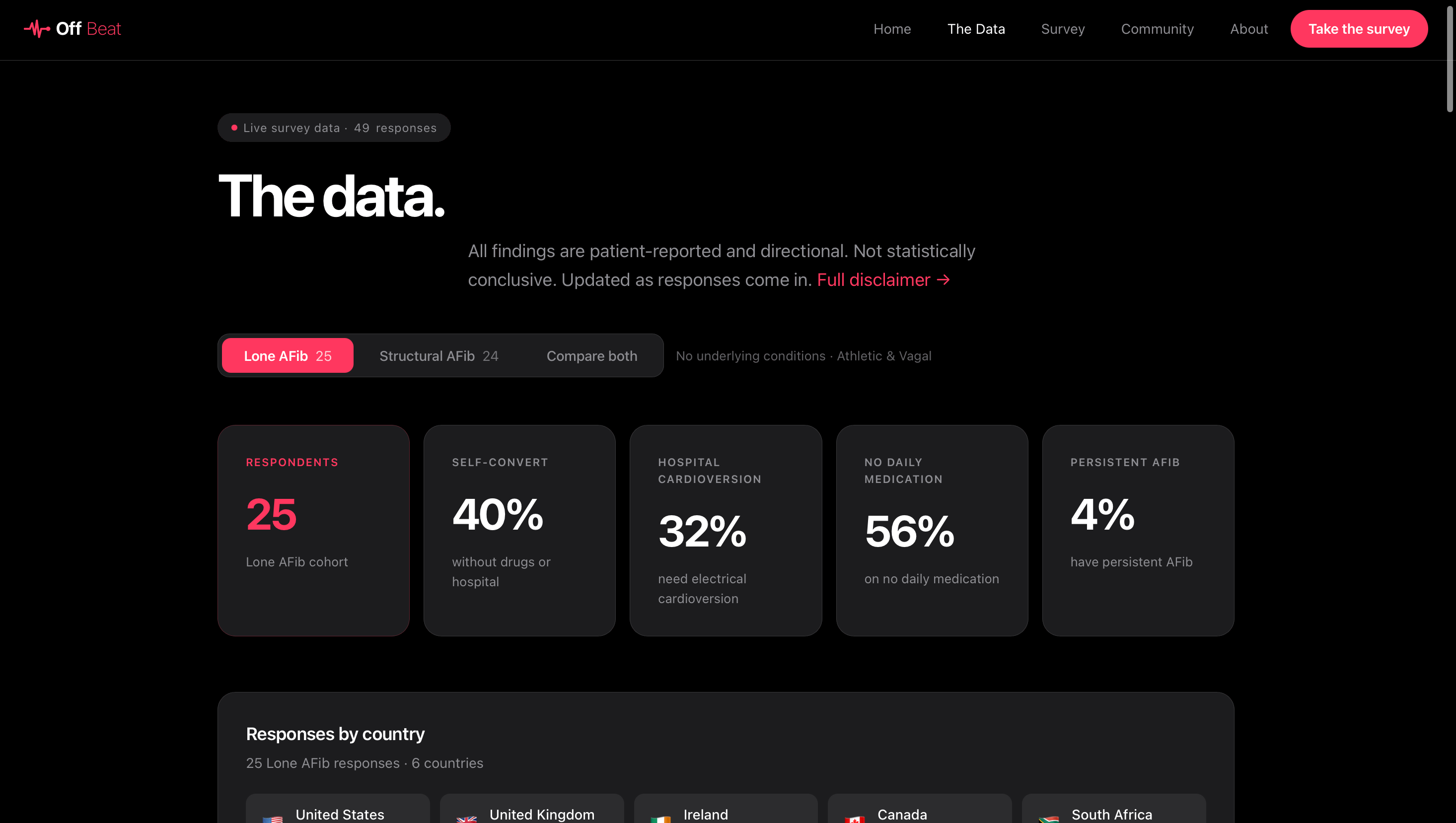
In early 2026 I launched Off Beat, a patient-led research platform for young, active people with AFib. The idea is simple: collect structured data from people who share this phenotype, visualise it in real time, and make it freely available.
It’s funded by nobody except the occasional generous person who buys me a coffee. We now have 49 responses from 8 countries. Here’s some of what we’ve found so far.
On fitness: 37% of respondents rate their fitness at 8-10 out of 10. This is not the typical AFib patient profile.
On medication: 56% of the Lone AFib cohort are on no daily medication. Most of us are managing this without long-term pharmaceutical intervention.
On ablation: 40% of the Lone AFib cohort have had an ablation, with an average satisfaction rating of 4.4 out of 5. That’s a striking finding, and one that’s hard to find anywhere in the published literature for this specific group.
On mental health: The average mental health impact score is 7.1 out of 10. Nearly two thirds of respondents report significant anxiety and mental health impact. We are living with something that medicine doesn’t fully understand, without good data to guide our decisions, and that uncertainty takes a toll that I don’t think gets acknowledged enough.
On triggers: Alcohol (36%), dehydration (28%), and emotional stress (28%) top the list for the Lone AFib cohort. Exercise triggers episodes in 20% of respondents, but for the majority of us, exercise is not the enemy.
Why this matters
Last month I wrote to Professor Marius Myrstad, who runs the NEXAF detraining study in Norway, one of the few research projects specifically focused on athletic AFib patients. He told me that patients with this phenotype are genuinely hard to recruit.
That’s the gap Off Beat is trying to fill. The goal is to build the largest dataset of young, active AFib patients in the world, not so academics can publish papers, but so that when you sit across from your cardiologist and ask what the evidence says about someone like you, there’s actually an answer.
What I need from you
If you’re a young, active person with AFib, or you know someone who is, please take the survey. It takes five minutes and every response makes the data stronger.
The survey is at offbeat.community/survey.
And if you find any of this useful, subscribe here. I’ll share findings as the dataset grows, along with anything else from the research world that seems worth your time.
We are not the standard AFib patient. It’s time we had data that reflects that.
Will Founder, Off Beat offbeat.community