


What 80 Young People with AFib Told Us (That No Clinical Study Would)
When I built Off Beat, I wanted data. What I got was something more uncomfortable than data.
I got 80 people — from New Zealand to Albania, across 11 countries — telling me what it actually feels like to have a heart that misbehaves. The numbers are striking. But the words are what stay with you.
“I used to live a happy outdoor-based lifestyle. Because of my AFib I have been anxiety-filled and cooped up. I miss my old self.” — Male, 30, United States
“It’s ruined my life and I live in fear.” — Female, New Zealand
“Feeling alone. I’m 34 and although ablations and arrhythmia issues are ‘common’ and ‘routine’, it’s not routine to me.”— Female, 34, United States
These are not outliers. These are the pattern.
The numbers first
Off Beat has now collected 80 survey responses from 11 countries. The respondents are young — average age at first episode is 32. Most are active, or were before diagnosis. None of them were supposed to have this.
Here is what the data shows.
About 60% stopped exercising entirely or significantly reduced their activity after diagnosis. For a population that largely defined themselves by movement — runners, footballers, cyclists, climbers — this is not a clinical footnote, it is an identity crisis.
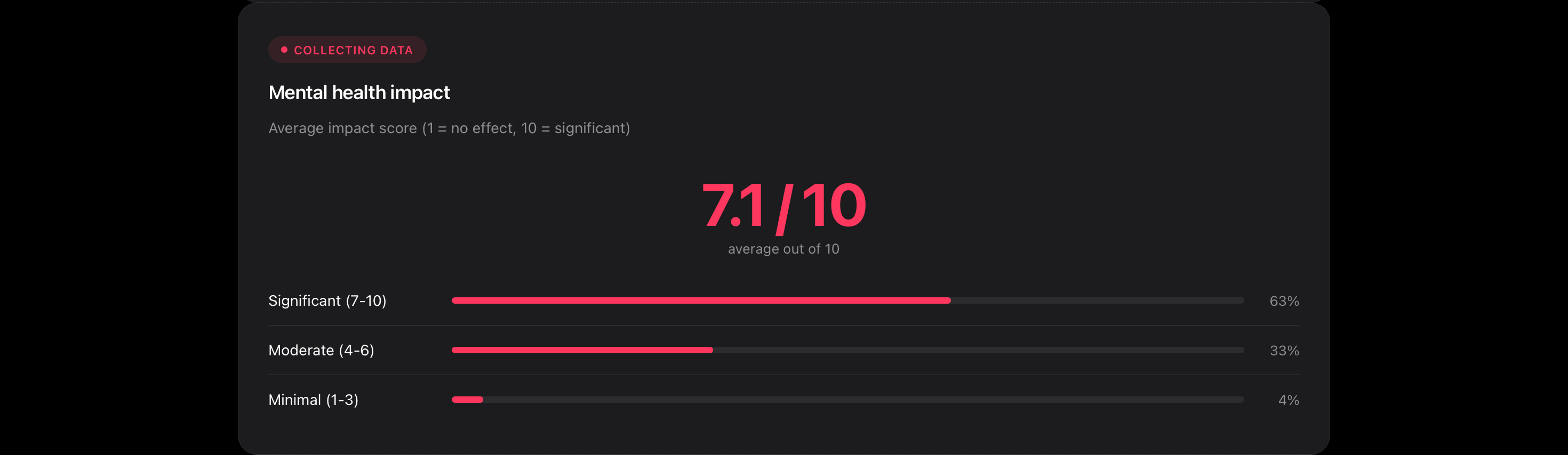
The mental health impact score averages 7.1 out of 10. Not 3. Not 4. Seven point one. And that is the average. Several respondents rated it 10 — the maximum — including people who by clinical measures are doing well. One episode every 13 months. No daily medication. Technically fine. “Sometimes I feel like my whole world is crashing down,” one respondent wrote, “when in reality I am continuing my day-to-day life as normal.”
The anxiety is disproportionate to the clinical severity. That is not a criticism of the people experiencing it — it is a finding. And it is almost entirely absent from the published literature on lone AFib management.
About 45% of respondents reported being dismissed by a doctor at some point. The exact phrasing from one submission: “My doctor told me that people my age don’t have heart issues.” He had over 400 recorded episodes by the time he received a diagnosis.
Wearables as the first line of diagnosis
Something unexpected emerged in the free-text responses. Multiple people described the same sequence: they had no idea anything was wrong, a wearable device flagged an irregular rhythm, and that flag — not a symptom, not a GP referral — was the beginning of their diagnostic journey.
“I had no idea of the issue. My watch told me about episodes when I slept. Led to a Holter, led to diagnosis and then ablation.” — Male, Australia
This is not reflected in any clinical pathway I am aware of. Consumer wearables are doing diagnostic triage for a condition that affects millions of undiagnosed people. That matters enormously. It also raises questions that nobody seems to be formally studying: what proportion of AFib diagnoses now originate from wearable devices? How accurate is that early detection? What happens to the people whose device flags something and their GP dismisses it?
The technology is ahead of the healthcare system. Our data is starting to show that.
The thing nobody talks about: pregnancy
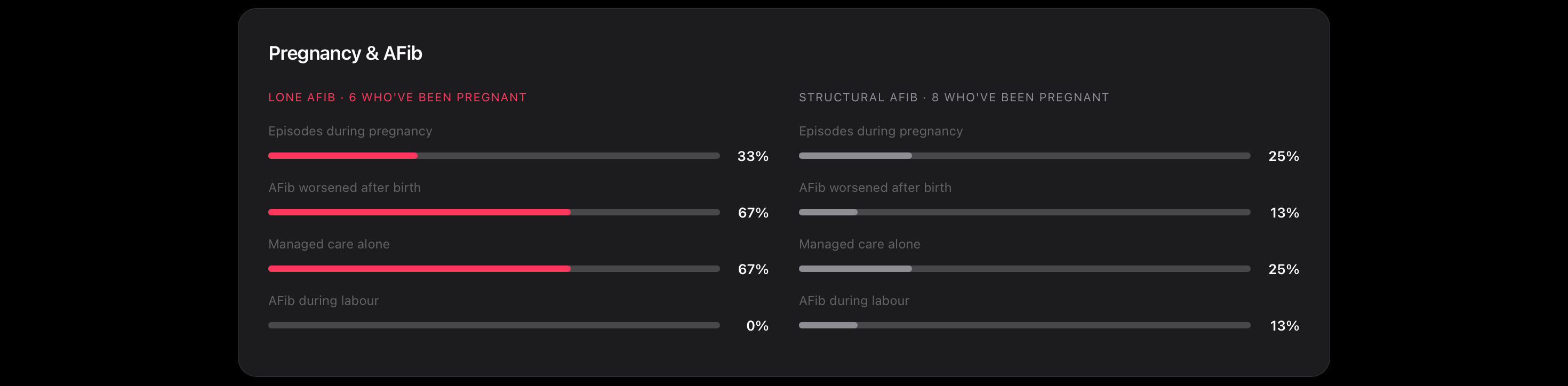
Of the female respondents who have been pregnant, 31% had AFib episodes during pregnancy. 38% report that their AFib got significantly worse after giving birth. And 46% managed their cardiac care during pregnancy largely alone — no joined-up care between cardiology and obstetrics, just a woman navigating two complex medical situations simultaneously.
“After giving birth I went into AF and have never left. In my early 30s as a new mum this has been horrendous. I have had next to no answers and just a long wait to see a cardiologist to even speak about what’s happening to me. It’s been 6 months of waiting so far.” — Female, 30, United Kingdom
She is still in persistent AFib. She submitted the survey this week.
What is actually helping
The data does offer some cause for cautious optimism. Magnesium supplementation, improved sleep, electrolyte management and reducing alcohol appear consistently in the responses from lone AFib respondents when asked what helps. These are not prescribed interventions, but things people figured out themselves, through community knowledge sharing, trial and error, and the kind of obsessive self-tracking that comes with having an unpredictable heart.
56% of lone AFib respondents are on no daily medication. That reflects both the pill-in-pocket approach many EPs favour for paroxysmal lone AFib, and the broader reality that this population is being managed conservatively — sometimes appropriately, sometimes because the system has not yet caught up with the scale of the problem.
40% have had an ablation. PFA dominates, with strong satisfaction scores. The people who have had it are, broadly, glad they did.
What I am building toward
Off Beat is not a study. It is a signal. With 80 responses from 11 countries, the data is directional — not definitive. But the patterns are consistent, and they are pointing at things that clinical research has not fully mapped.
The average age at first episode in this cohort is 32. The existing published literature on AFib skews heavily toward patients in their 60s and 70s. The drugs, the risk models, the quality-of-life frameworks — almost all of it was built for a different patient. We are trying to understand a condition using tools designed for someone else.
That is what Off Beat is trying to change. One survey response at a time.
If you have AFib and haven’t taken the survey: offbeat.community/survey. It takes 5 minutes and every response makes the picture clearer.
If you are a researcher, clinician or journalist who wants to discuss what this data is showing: hello@offbeat.community.