

From the ER to a PR: How I Got Back to Running After AFib, and How You Can Too
On 3 January 2026, I ran 21 kilometres (13.1 miles) through the Surrey Hills on one of those perfect winter mornings that make you glad to be a runner. Crisp, cold, sunny, with a feels-like temperature of -7C (19F). The kind of cold that makes your lungs sharp and your legs feel light. These hills in Surrey are where they filmed the Bond movie, Skyfall (pretending it was the Scottish Highlands). They’re genuinely beautiful, and that morning they looked it. My average heart rate was 159bpm, my max hit 176, I climbed 458 metres, and I burned 1,737 calories. I felt exactly like someone in the shape of their life.

Four days later, I was in the emergency room.
My heart had gone into atrial fibrillation. Three nights in hospital. The threat of cardioversion. My heart eventually found its way back to sinus rhythm on its own, helped along by beta blockers, but not before I’d had a lot of time to stare at a ceiling and wonder whether I’d ever run like that again.
Five months and three days after being discharged, I set a 10K personal record.
I’m not writing this to show off about that. I’m writing it because when I was lying in that hospital bed, I couldn’t find anyone who had documented what coming back to exercise actually looked like. The forums were full of conflicting anecdotes. The clinical advice was general. Nobody had shown the specific shape of the journey: the weeks, the distances, the heart rate numbers, the nights that were hard, and the runs that slowly rebuilt confidence.
This is that document. It’s my journey, but the lessons belong to anyone trying to find their way back.
What the gap actually looks like
After the half marathon, I didn’t run again for 37 days.
If you’ve just had a cardiac episode and you’re wondering when you’ll feel like yourself again, 37 days is a useful number to have. Not because it will be exactly 37 days for you, but because it gives you a sense of scale. We’re talking weeks, not months. And the return isn’t linear.
The Strava data is clean about the gap: one entry on 3 January, then nothing, then 9 February. What the data doesn’t capture is what those 37 days felt like.
In the first week out of hospital I was getting ectopic beats around five times a day. If you don’t know what ectopics feel like: imagine your heart briefly forgetting its rhythm, a thud or a skip or a sensation like something flipping in your chest. They’re usually harmless. They don’t feel harmless when you’re scared you might end up in hospital again. I also had air hunger, a persistent sense of not being able to take a full breath even though my lungs were working fine. I felt winded going upstairs.
The second week was more settled. But the nights didn’t improve. On 17 and 18 February I kept waking between 1 and 3am with a strange dropping sensation in my chest, almost like weightlessness, that lasted about an hour before fading. And on 23 February, out on a walk, I had a fluttering sensation that convinced me I was about to go back into AFib.
I made a note on my phone that night:
“I’ve ‘recovered’ now a month and a bit on, but am still getting ectopics and waking up in the night worried I’m about to go back into AFib. I’ve run a bit since going into hospital and have been fine during, but am conscious that I’m having more ectopics at night time, likely because I’ve exerted myself during the day.”
I’m including this because if you’re having these experiences right now, I want you to know they were part of my recovery too. They don’t mean something is wrong. They mean your nervous system is catching up with your body.
Step one: get the actual evidence
The single most important thing I did before returning to exercise was get a complete clinical picture of my heart. Not reassurance. Evidence.
My electrophysiologist, Professor Malcolm Finlay reviewed everything in late February: a cardiac MRI, an echocardiogram, blood tests, and Apple Watch ECG traces I’d been sending through. The cardiac MRI was completely normal. No inflammation in the pumping chambers, no evidence of narrowed arteries, no microvascular issues. The echocardiogram was normal. The blood tests were normal.
His written conclusion: “Your heart is in an excellent state structurally. You can continue with your normal activities, including exercise. You should feel confident in your health.”
Those words mattered not because a specialist said them, but because they were grounded in actual evidence. The MRI, the echo, the bloods: these weren’t platitudes. They were data. And the data said the heart was structurally sound.
This is the non-negotiable first step for anyone returning to exercise after a cardiac event. A specialist who has looked at your specific heart and can tell you what it actually shows. Everything I’m about to describe only makes sense in the context of that clinical clearance. Get yours before you lace up.
The day after that consultation, 25 February, I ran 5km (3.1 miles) in the sun past Buckingham Palace. I made a note:
“It’s the first time the sun has shone this year, and I feel so much better for it. My doctor told me that all my tests were normal yesterday, which I was expecting, but was reassuring to hear anyway.”
Step two: answer the question honestly
There’s a question every active person with a cardiac condition eventually has to sit with. I think it’s better to name it directly than to dance around it.
The question is: knowing that exercise may be a trigger for your condition, do you still want to do it?
Here’s how I answered it, in my own notes at the time:
“I decided to run today because I’d rather run, enjoy it, and potentially put myself at a higher risk of going back into AFib, than give up something I now love doing and that keeps me fit and healthy, in every way apart from potentially triggering AFib.”
Your answer may be different. But it has to be yours. The version of this story where I gave up running is not a safer story. It’s just a different one. Whatever you decide, decide it consciously rather than letting fear make the decision by default.
Step three: start smaller than feels necessary
On 9 February, 37 days after the half marathon, I ran this:
2.5K: AFib Recovery Run ❤️🩹 1.56 miles. Average HR: 129bpm. Max HR: 167bpm.

Fifteen minutes. Flat ground. Slow pace. I watched my watch the entire time.
That average heart rate of 129bpm was around 30 beats per minute lower than my half marathon pace. I wasn’t training. I was testing.
Start here, or somewhere like here. Start at the distance and pace that feels almost embarrassingly small for someone at your fitness level. The ego cost is real. The cost of coming back too hard and having a scare, and then having to rebuild the psychological ground all over again, is higher.
The run was fine. I went home and felt, for the first time in five weeks, like myself.
Step four: let the data build the case
Here is the rebuild, month by month. June figures run to 14 June only.
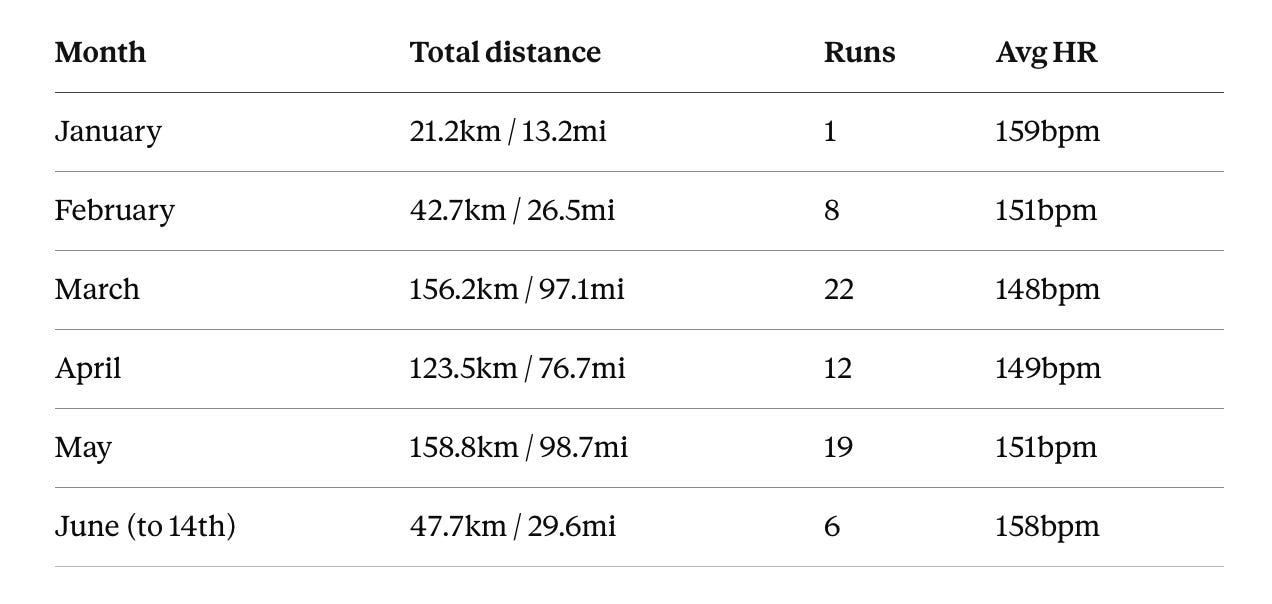
Look at the jump from January to March. One run at 21km, six weeks of nothing, then 156km across 22 runs in a single month. On paper it looks sudden. In reality it was incremental: each run a small test that the previous one had made slightly easier.
February: conservative by design. Eight runs, all easy. Heart rate deliberately low. The progression went 2.5km, 5km, 5km, 11km over roughly two weeks, with rest days in between. If you’re early in your return, this shape is worth copying. Short, frequent, low-intensity. Prove to yourself that the body works, then ask more of it.
March: when trust comes back. 156km across 22 runs. I started running with other people again. The runs had names in them, friends I was meeting, routes we were sharing, conversations that had nothing to do with AFib. Running had stopped being a medical exercise and started being ordinary again.

On 29 March I ran 15km (9.3 miles) with 355 metres of climbing at 153bpm average heart rate. Six weeks after my first 2.5km shuffle.
Heart rate as your ongoing evidence. One of my quiet anxieties through the early weeks was whether my heart rate would behave differently after the episode. The data says no. By March my average running HR was lower than during the half marathon, reflecting easier effort levels. The max heart rates, 173, 174, 180, were consistent with pre-episode figures. Each session that produced normal heart rate data was another data point in the case for being okay. Watch yours. Let it tell you the same thing.
April: real distances return. Two runs at 16km (10 miles) and 16.5km (10.3 miles). A 14km (8.7 mile) climb. By this point I’d largely stopped thinking about the episode mid-run. Not because I’d forgotten it, but because the body had been generating its own evidence for two months, and the evidence was consistently good.
Step five: let the performance follow
On 5 May 2026, four months after the hospital stay, I set a 5K personal record.
5K PR: 20:25 (4:05/km or 6:33/mile pace) Average HR: 167bpm. Max HR: 180bpm.
Then, on 11 June 2026:
10K PR: 43:51 (4:23/km or 7:03/mile pace) Average HR: 167bpm. Max HR: 177bpm.
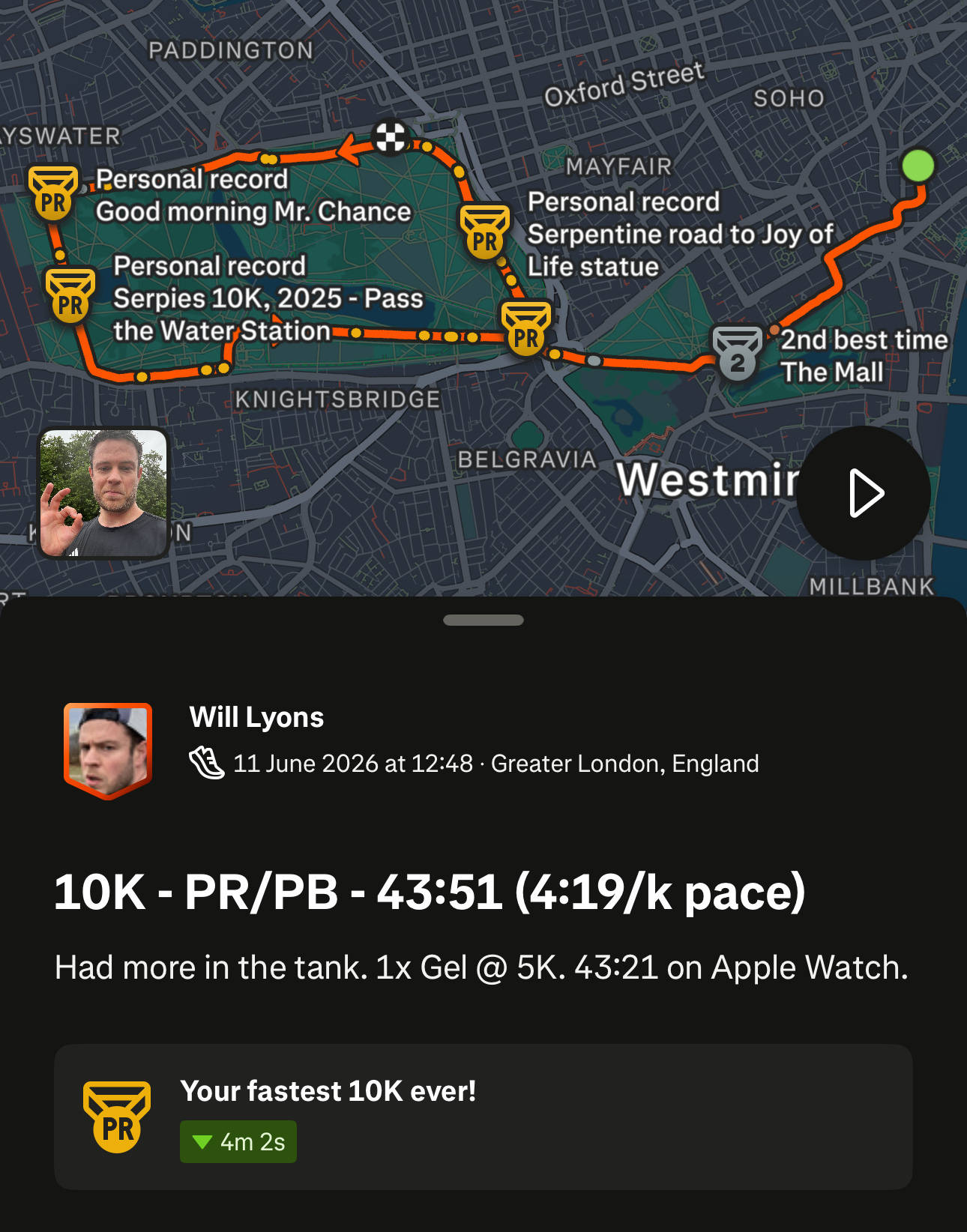
I’m including these not as personal achievements but as evidence. The heart that was in the emergency room in January was setting personal records in June. That heart is structurally normal. It responds to training. It performs under load. The data says so.
From the ER to a 10K PR in 159 days.
If you’re at the beginning of your return right now, this is what 159 days of patient, data-informed rebuilding can produce.
When it stops feeling like a recovery
By mid-May I made a note that read: “My heart feels completely normal now and I am running a lot, which I’m enjoying.”
There was no single moment when the recovery ended and ordinary life resumed. It was more like a gradual fading: the anxious night-time awareness slowly replaced by the ordinary background hum of being someone who runs. The ectopics were still there sometimes. But the relationship with them had changed. They were information rather than threat.
This shift from hypervigilance to ordinary awareness is probably the least-discussed part of returning to exercise after a cardiac episode. The body heals faster than the nervous system does. The Strava data was telling me I was back months before my brain fully believed it.
Your nervous system will catch up. Give it time, and give it data.
The practical summary
Get actual evidence first. An MRI, an echo, a proper clinical picture of your specific heart. Not reassurance: evidence. This is the non-negotiable step.
Answer the question honestly. Do you still want to exercise, knowing the risk? Answer it consciously. Don’t let fear answer it for you by default.
Start smaller than feels necessary. Something like 2.5km (1.5 miles) at a gentle pace with your HR monitor on. The distance doesn’t matter. The habit of going out and coming back fine does.
Use your data as your evidence base. Every session that ends normally is a data point. Watch your heart rate. Let it reassure you. Then gradually stop needing to watch it quite so closely.
Run with people. When you’re ready. It moves your attention away from your chest, and it means you’re not alone if something does go wrong.
Don’t rush the long stuff. Distance before intensity. Easy long runs before hard short ones. Give your body time to prove itself at volume before you push it on pace.
Accept the days the fear wins. They’ll happen. They won’t show up in the data. They’re part of it anyway.
The fear doesn’t fully disappear. I still notice things I didn’t notice before January. A skipped beat during a hard effort. A heart rate that starts a little high. But the relationship with those observations changes as the evidence accumulates. Every run that ends normally is one more data point confirming that your body knows what it’s doing.
Five months after the ER, the data says everything is fine.
It’s probably trying to tell you the same thing.
Will Lyons is the founder of Off Beat (www.offbeat.community), a patient-led research platform collecting data from younger, active people with AFib. More than 120 people across 14 countries have shared what this condition looks like in people like them. If you’re under 50 with AFib, your data helps others find their own way back.